Should You Take Vitamin D for COVID-19 Protection?
COVID-19 and Vitamin D – What’s Hype, What’s Real
We wanted to know if vitamin D supplementation could help prevent and fight COVID-19 infection. So we hit the books, did the research, and here are the results—provided as a resource to help you decide if vitamin D supplementation is right for you.
Since the early days of the pandemic, I have been closely following the research on the relationship between vitamin D and COVID-19. And now, a solid 8 months into the pandemic in the US, this relationship has become somewhat of a trending topic, brought on by a few select headlines in international newspapers. These trending articles state that vitamin D deficiency was found in 80% of COVID-19 patients. Researchers Dieter de Smet, DM (et al), after analyzing the data, state that:
Vitamin D deficiency is a prevalent risk factor for severe COVID-19. Vitamin D supplementation might be an inexpensive and safe mitigation for the SARS-CoV-2 pandemic.
This is compelling research and makes for a great news headline, but what does it actually mean? And should you be supplementing with vitamin D?
Let’s review the literature together, but before that, let's first review what exactly the SARS-CoV-2 virus in, learn a little bit more about the immune system, including innate, adaptive, and innate immunity, and then move on to vitamin D and the if there is a gain to vitamin D supplementation in supporting the body to both prevent and fight COVID-19 infection.
Before we get to reviewing the literature, it is important to emphasize that knowledge here is in its infancy. It is emerging. It is imperative to emphasize that we are not presupposing that vitamin D—or anything—prevents or cures COVID-19. According to the best reading of the current literature, as we will see below, it appears that vitamin D helps prevent infection and supports the body in fighting infection. This is very different from stating that it will prevent infection or that it will cure infection. Now on to the science.

COVID-19 – The Global Pandemic and Global (Dis)Infodemic
There is a flood of information, misinformation, interpretation, and misinterpretation. As a result, it is difficult for any of us to determine which information is accurate and which of that is applicable to us. By its very nature, a pandemic is dynamic and confusing. Remember when we were unsure whether or not to sanitize groceries as they came into the house?
What appears true now may become obsolete within an hour. We need to learn, revise, adapt, and then repeat—applying the scientific method to our consumption of media. Adding to the confusion is severity: With this pandemic, the consequences of false claims, misinformation, and misinterpretation prove grave. Life threatening.
Sanitizing groceries, while a hassle, is ultimately benign. But let us not forget when the malaria drug hydroxychloroquine (Plaquenil) was touted as a magic bullet. Deaths were the result of this misinformation, and since then, hydroxychloroquine has been associated with higher death risk in COVID-19 patients.
Update: On November 9th, the American Medical Association published primary research on the effectiveness of hydroxychloroquine in the treatment of COVID-19. Through a randomized clinical trial, comprised of "479 hospitalized adults with respiratory symptoms from COVID-19," researchers conclude that:
Among adults hospitalized with respiratory illness from COVID-19, treatment with hydroxychloroquine, compared with placebo, did not significantly improve clinical status at day 14. These findings do not support the use of hydroxychloroquine for treatment of COVID-19 among hospitalized adults.

A Quick Overview of Viruses, Coronaviruses, and SARS-CoV-2
At its most basic, a virus is a tiny parasite. Within microbiology, there is even debate as to whether a virus is even a living organism, with the consensus trending toward no. Viruses are composed of either DNA or RNA surrounded by a shell of protein (it is this protein shell which earns coronaviruses their name). Viruses divide only inside the living cells of an organism. They have no capacity to reproduce outside of a host.
Viruses can infect humans, animals, plants, and bacteria. Some viral diseases in humans are:
- Flu;
- Common cold;
- Parainfluenza virus infection;
- COVID-19;
- Measles;
- Smallpox;
- Herpes;
- AIDS.
Coronaviruses – An Emerging Global Health Threat?
Coronaviruses represent a family of related RNA viruses. They usually cause mild respiratory illnesses, such as the common cold.
Of hundreds of coronaviruses found in different animals, only seven are known to cause illnesses in humans:
- 229E (alpha coronavirus);
- NL63 (alpha coronavirus);
- OC43 (beta coronavirus);
- HKU1 (beta coronavirus);
- MERS-CoV (Middle East Respiratory Syndrome; MERS);
- SARS-CoV (Severe Acute Respiratory Syndrome; SARS);
- SARS-CoV-2 (Coronavirus Disease 2019; COVID-19).
Four of these viruses (1-4) cause only mild to moderate disease. Nevertheless, the last three of these viruses (5-7) can cause severe or even fatal infections.
MERS-CoV, which jumped from camels to humans, has caused 2494 cases of illness and 858 deaths. The MERS outbreak started in September 2012 and continues to cause limited outbreaks.
SARS-CoV, which probably came from civets or ferret-badgers, affected 8089 people and caused 774 deaths globally. The outbreak began in November 2002 and has not been detected since 2004.
As of writing this article, SARS-CoV-2 has affected over 45 million people and caused 1.1 million deaths globally. The first case was reported to the WHO on December 31, 2019.
Researchers think the outbreak started from a seafood market in Wuhan, Hubei Province, China. It is not clear whether the virus jumped from a bat, snake, or pangolin.
The WHO declared the outbreak a Public Health Emergency of International Concern (PHEIC) on January 30, 2020. On March 11, 2020, it declared COVID-19 a global pandemic.
Understanding the Functions, Parts, and Types of the Immune System
To better understand how vitamin D may support the immune system in preventing and fighting COVID-19 infection, it is important to understand that there is not an immune system; rather, the immune system is a collection of systems which work in harmony. Each and every day, we touch, eat, and breathe in millions of infectious organisms. However, not everyone who is exposed to germs develops the infection. It is because we all have some level of immunity.
The immune system protects us against attack by potential pathogens. A myriad of cells, tissues, and organs work together to help fight infection. For the most part, when speaking of the immune system and immunity, we tend to think of immune cells. Immune cells—with the exception of autoimmune disorders—attack only those particles that they perceive as harmful. These particles are known as antigens.
When an antigen invades the body, the immune cells attack it. This is known as an immune response. During the response, specialized immune cells produce proteins to fight and destroy the germs. These proteins are called antibodies.
Some immune cells, known as B cells, record the type of microorganism. Thus, when the same germs attack again, your body quickly releases antibodies specific to them.
Here, we see a straightforward progression of immunity: Some type of infectious agent enters the body, immune cells recognize this agent based on their antigens, the body produces antibodies to fight the infectious microbe, and specialized immune cells remember what that infectious agent (antigen) looks like so in the future it can fight it again.
But the immune system is much more than this.
Immune System is Made of Cells, Tissues, and Organs
The immune system is made up of:
- The Skin – Acts as a barrier that prevents germs from entering the body;
- Mucous Membranes (Mucosae) – The thin, moist layers of cells that line the inside of organs and body cavities. They produce mucus that can trap microorganisms and thus help prevent infection;
- White Blood Cells (Leukocytes) – Kill bacteria, fungi, and other parasites. Some leukocytes produce antibodies (proteins) against specific bacteria and viruses;
- The Lymphatic System – Produces and carries leukocytes and other immune cells. The lymphatic system includes the thymus, spleen, tonsils, lymph nodes, lymph vessels, and bone marrow.
Three Types of Immunity
- Innate immunity – Innate immunity protects you right from your birth. Also called natural immunity, it is the body's first line of defense. This type of immunity is non-specific and works as general protection against potentially dangerous substances. For example, the intact skin and mucosa prevent germs from entering the body.
- Adaptive immunity – This type of protection is also called acquired or active immunity. It typically lasts for longer durations. You develop adaptive immunity when you are exposed to disease-causing germs or vaccinated.
- Passive immunity – This short-term immunity lasts only a few weeks or months. Passive immunity involves antibodies that you get from an external source. For example, you get antibodies from your mother’s milk right during breastfeeding. These antibodies work immediately, but the effects wane rapidly.
At the end of this article, we will touch upon the Swiss cheese respiratory pandemic defense. And I would add here that the immune system can be taken even farther than the physiological components above: There are actions and behaviors that we can take to bolster our innate immunity.
Our Immune System Doesn’t Know What to Do With the COVID-19 Virus
SARS-CoV-2 is a novel coronavirus. Being novel means that the virus is being seen in humans for the first time. This is an important differentiation between SARS-CoV-2 (COVID-19) and other viruses that we come in routine contact with, such as the common cold or flu.
When the immune system encounters a novel virus, it does not know what to do with it. In essence, the immune response is not similar to what would have happened to a known germ.
The immune cells are overwhelmed and release excessive inflammatory chemicals, known as the inflammatory cascade or the cytokine storm. This explains why people with COVID-19 are more likely to develop a hyperinflammatory state that often leads to acidosis, sepsis, severe lung damage, multiorgan failure, and blood clotting disorders.
These people need treatment in an intensive care unit (ICU). Several studies show that sepsis is the leading cause of death in critically ill patients. Sepsis is a fatal condition in which the body’s immune system attacks the patient’s own tissues.
A 2020 PloS One study reveals that the majority of SARS-CoV-2 deaths are caused by:
- Acute respiratory distress syndrome (ARDS). It causes a rapid loss of respiratory function following widespread lung inflammation;
- Sepsis;
- Multiple organ failure;
- Excessive bleeding;
- Kidney failure;
- Heart failure.
The study also noted that people above 60 and with long-term diseases were more likely to die from the infection. The most prevalent chronic diseases in those who died were diabetes, heart disease, and high blood pressure.
Update: On November 11th, the Journal of Ultrasound Medicine published their findings regarding COVID-19 "acute testicular infection." Looking at ultrasounds of 142 hospitalized in patients with COVID-19, researchers found evidence of high rates of testicular infection, with higher rates of infection tied to increased age.
Our results lend credence to the idea that SARS‐CoV‐2 infection may specifically affect the testis, epididymis, or both...we suggest that clinicians remain aware of the risk of acute scrotal infection in hospitalized patients with COVID‐19, and for young male patients with COVID‐19, especially those who wish to have children, local symptoms and fertility should be carefully monitored and protected.
In the publication, the researchers note that because the study only included ultrasound scans, it is impossible to state whether the evidence of infection was due to a co-morbidity, to specific accumulation of COVID-19 infection in the testes, or a result of immune response and inflammation resulting from COVID-19 infection.
We are choosing to include this study here because a large percentage of our customer base is interested in male reproductive health and fertility.
Vitamin D Might Help, But There is a Catch
Vitamin D is a fat-soluble vitamin. Our skin makes vitamin D when it is exposed to the sun’s ultraviolet rays. Under ideal conditions, the body will synthesize about 80% of the total vitamin needed in the body. However, this is dependent on location and time of year. In the northern hemisphere, those living above the 37th parallel of latitude will only be able to synthesize vitamin D for several months out of the year. The 37th parallel cuts horizontally from just below San Francisco to Richmond, Virginia.
The New England Journal of Medicine provides real-life examples illustrating the influence of geography and season on the body’s ability—and inability—to synthesize vitamin D from sun exposure. In the article “How Much Sunlight Is Equivalent to Vitamin D Supplementation?” the authors write:
At noon in Miami, someone with Fitzpatrick skin type III would require 6 minutes to synthesize 1000 IU of vitamin D in the summer and 15 minutes in the winter. Someone with skin type V would need 15 and 29 minutes, respectively. At noon in the summer in Boston, necessary exposure times approximate those in Miami, but in winter, it would take about 1 hour for type III skin and 2 hours for type V skin to synthesize 1000 IU of D. After 2 PM in the winter in Boston, it is impossible for even someone with Fitzpatrick type I skin to receive enough sun to equal even 400 IU of vitamin D.
Vitamin D Synthesis and the Fitzpatrick Scale
The Fitzpatrick Scale (developed by dermatologist Thomas B. Fitzpatrick) is a model used to classify skin type based on its reactivity to UV exposure. In the above example, Fitzpatrick skin type III, sitting directly in the middle of the six types, is described as skin that is white and prone to mild burns but uniform tanning. Fitzpatrick type V is dark brown to black and rarely burns and tans rapidly. It is important to note two things here. Firstly, that the scale was developed—and is employed here—specifically to better understand UV exposure on the range of skin pigmentation. Secondly, and perhaps most important to this discussion, that lighter skin color is the result of genetic mutations, which were evolutionarily selected for because the lighter the skin color the more rapidly it can synthesize vitamin D.
The applicability in this discussion is the inverse relationship between skin pigmentation and vitamin D synthesis: The more pigmentation the skin has, the less vitamin D it synthesizes. At lower latitudes this may not matter; at higher latitudes, it does.
In the US, there is an undeniable and tragic racial disparity in those hardest hit by COVID-19, with African American communities experiencing an infection rate three times higher than communities of predominantly white Americans. The death rate within African American communities is six times higher than in predominantly white communities. While in no conceivable way can this disparity be explained away by one’s ability to synthesize vitamin D, it does perhaps support the assertion that low vitamin D levels both make one more susceptible to COVID-19 infection and less capable to mount an effective immune response to it.
Without the right sun exposure and supplementation, vitamin D can be obtained from dietary sources, such as:
- Liver oil;
- Fatty fish;
- Beef liver;
- Fortified dairy;
- Egg yolk;
- Mushroom.
There are two forms of supplemental vitamin D:
- Cholecalciferol (Vitamin D3);
- Ergocalciferol (Vitamin D2).
Vitamin D and Your Immune System
Most people are familiar with the role of vitamin D in healthy bones and teeth. But the vitamin impacts many systems throughout the body, including the endocrine system, where it is known as a master hormone, and it is a potent modulator of the immune system.
Immune cells—both B cells and T cells—require the vitamin’s active form, and vitamin D deficiency has been consistently associated with an increased risk of infection. But is there a relationship between vitamin D and COVID-19 infections?
While we’re still learning, the answer is yes (with a caveat).
In August, a team of researchers in Spain studied the link between intensive care unit (ICU) admissions and vitamin D supplementation.
They found that COVID-19 patients who received a vitamin D analog (calcifediol) with other drugs had significantly lower ICU admissions than the non-vitamin D group (2% vs. 50%).
While the results were promising, the study had major limitations. For example, it was a small study and did not consider other factors that might have influenced the results. These include existing health issues in participants and vitamin D levels before and during the study.
Moreover, one should note that the researchers used calcifediol, not cholecalciferol. Calcifediol is more rapidly absorbed than cholecalciferol.
So while the answer is Yes, the caveat is that we still need more information before making an absolute assertion.
Vitamin D Is a Master Antioxidant
Above, we see that in very specific ways, vitamin D supports immune system health. There is an undeniable, dependent relationship between vitamin D levels and immune function. Below, we will see how in very specific ways, vitamin D modulates how SARS-CoV-2 is able to—or rather not able to—infect the body and how vitamin D modulates the body’s response to SARS-CoV-2 infection.
Nonspecific to COVID-19, vitamin D is a master antioxidant. While this post would become a multi-volume dissertation if it addressed all the roles, functions, and benefits of vitamin D, in fighting and healing from illness, the antioxidant potential of vitamin D should not be glossed over. In fact, vitamin D is able to cross the blood-brain barrier and support glial cells. Glial cells are the “support cells” to neurons, and can be found throughout the central nervous system (which includes the brain and spinal cord) and the peripheral nervous system.
Glial cells are not just one type of cell, rather, they include six different types of cells, all of which work within four main supportive functions:
- Physical/structural support to neurons;
- Nutrient and oxygen support to neurons;
- Producing myelin (insulating factor for neurons);
- Immune function, including protection from pathogens.
We know that neurological symptoms are a tell-tale of COVID-19 function, including impairments on taste and smell, “foggy head,” and that neurological systems are persisting into long COVID. We’re also seeing mental health issues presented in long COVID. All of this is relevant in the discussion of vitamin D as an antioxidant and in the prevention of COVID-19 infection and in the immune response to it.
Update: On November 9th, 2020, Reuters published an article titled, "One in 5 COVID-19 patients develop mental illness within 90 days." The Reuters article was reporting findings in The Lancet Psychiatry journal, which reviewed 69 million electronic health records of Americans, which included more than 62,000 cases of COVID-19.
Based on the health records, researchers found that within "the three months following testing positive for COVID-19, 1 in 5 survivors were recorded as having a first time diagnosis of anxiety, depression or insomnia...about twice as likely as for other groups of patients in the same period." For those with a history of diagnosis, that occurrence grew to 61%.
Vitamin D and COVID-19 – What the Science Says So Far
- Preliminary evidence shows that vitamin D deficiency may increase COVID-19 risk.
- Notably, one recent study found that over 4 out of 5 people with the disease were deficient in vitamin D.
- A large study found that low vitamin D levels could increase the risk of getting COVID-19 by about 50%. The same study noted that supplementation might help prevent respiratory infections, especially in those who are deficient.
- Vitamin D deficiency could contribute to acute respiratory distress syndrome (ARDS). ARDS affects about 15 percent of COVID-19 patients and is responsible for up to half of all COVID deaths.
How Vitamin D Might Help Prevent COVID-19 or Its Complications
Vitamin D is a master hormone and regulator in the body. Its importance is wide-spread and not limited to immune function. However, when it comes to immune function, it is vital to note that irrespective of COVID-19, vitamin D regulates both innate and adaptive immunity.
ACE-2 Receptors and How Vitamin D May Help Prevent COVID-19 Infection
SARS-CoV-2 enters the body by attaching itself to ACE-2 (angiotensin-converting enzyme 2) receptors. These receptors are the doorway that the virus uses for entry into the body. Vitamin D prevents the virus from entering cells by blocking ACE-2 receptors. This is not just locking the door, but essentially locking and hiding the door.
This is incredibly important and should not be overlooked. The novel coronavirus must attach to ACE 2 before they enter into the cells.
Vitamin D and the Cytokine Storm
Additionally, vitamin D supports the innate immune system by maintaining a healthy balance between pro-inflammatory and anti-inflammatory cytokines. As we will see, this proves especially important in regulating the immune response to the novel coronavirus.
When a pathogen enters the body, the innate immune system produces two types of cytokines (proinflammatory and anti-inflammatory). SARS-CoV-2 infection results in a surge of proinflammatory cytokines: interferons, interleukins, tumor-necrosis factors, and chemokines, and an increase in proinflammatory angiotensin II.
This overactive immune response is known as the cytokine storm and is a major cause of complication and death in COVID-19 patients. The cytokine storm can result in ARDS, severe pneumonia, multiple organ failure, and abnormal blood clotting.
Vitamin D Upregulates ACE-2 Receptors
Vitamin D upregulates ACE-2 receptors (while this may seem counterintuitive, please read on). ACE-2 receptors are involved in converting proinflammatory angiotensin II into smaller proteins which are actually protective of the lungs, helping to clear proinflammatory compounds which may promote acute respiratory distress and thus decreasing lung injury. In animal models, COVID-19 infection has been shown to downregulate ACE-2 receptors, thereby reducing the body’s capacity to regulate angiotensin II.
As ACE-2 receptors are breaking down angiotensin II (which is harmful), the smaller proteins (peptides) produced are antimicrobial and line the respiratory tract. Two of these peptides are cathelicidin and defensins. Research shows that these peptides reduce the development of COVID-19 symptoms.
Above we learned that ACE-2 receptors are the entryway for COVID-19 to enter the body, so would it not reason that upregulating those receptors would be a bad thing? Well, no, because vitamin D, while upregulating them, is blocking the virus from finding and entering them. With vitamin D supplementation, the receptors are still available—at an increased capacity—to perform their job of breaking down proinflammatory angiotensin II while at the same time preventing COVID-19 from entering the body.
Vitamin D reduces pro-inflammatory cytokine levels and increases anti-inflammatory cytokine levels. It controls the adaptive immunity-induced inflammatory response in two ways. This is important not just for COVID-19 infections, but for all of us, all the time.
- Vitamin D suppresses the production of inflammatory cytokines: interleukins and interferon gamma;
- Vitamin D enhances the production of T regulatory cells (Tregs). Tregs regulate the immune response to the coronavirus.
Vitamin D and Vitamin C
The role of high dose vitamin C supplementation on COVID-19 is currently being studied and there is promising preliminary evidence to suggest a COVID-19 specific benefit to vitamin C supplementation. Vitamin D supplementation helps maintain vitamin C reserve in the body.
To recap, vitamin D:
- Blocks entry of COVID-19;
- Decreases proinflammatory cytokines;
- Increases the body’s ability to regulate the cytokine storm (proinflammatory angiotensin II) which leads to respiratory distress;
- Increases the production of beneficial cytokines and other peptides which can reduce COVID-19 symptoms;
- Supports the body’s vitamin C reserves.
Finding the Sweet Spot – A Look at What We Know and What We Don’t
Vitamin D is generally safe and accessible, with benefits far beyond any role it may play in preventing or decreasing the effects of COVID-19 infection. In the past we have written extensively about Vitamin D, including the influence of vitamin D on testosterone production and sex hormone binding globulin and how to safely repair and raise vitamin D levels.
As mentioned, the vast majority of those living in the US live above the 37th line of latitude, meaning that for the vast majority of the year, they cannot synthesize vitamin D from sun exposure. Estimates suggest that:
- Over half of nursing home residents and hospitalized patients are deficient.
- 47% of African American infants and 56% of Caucasian infants have low levels of the vitamin.
Thus, supplementation can help fight deficiency and associated adverse effects, such as the increased risk of falls and infections.
Again, it is important to note that caveat: We’re still learning. While the evidence is strong as to the benefits of vitamin D on SARS-CoV-2 infection, there are things that we still do not know. These include:
- No established positive effects in a large population;
- A lack of well-established dose for COVID-19;
- No well-controlled studies;
- Studies have not yet found the exact mechanism through which supplementation could benefit COVID-19 patients.
Moving Forward – What to Consider
Consider the following if you are thinking of supplementing with vitamin D specifically because of COVID-19:
- Vitamin D3 supplementation, daily or weekly, at daily equivalent doses of 1000–4000 IU, is recommended.
- For most people, daily doses may be more effective than mega doses.
- Depending on location and time of year, exposure to sunlight and sufficient vitamin D levels might reduce risks for both COVID-19 cases and mortality.
- Increasing age and co-occurring chronic diseases increase the risk of death. Lower vitamin D levels are common in older adults and those with chronic conditions.
- To reduce the risk of infection, experts recommend people at high risk consider taking 10,000 IU per day of vitamin D3 for a few weeks, followed by 5000 IU per day.
- For those who have already caught the infection, higher vitamin D3 doses might be useful.
Moving Forward – The Takeaways
- There is no cure for COVID-19. The only measures to avoid catching the virus are social distancing, masks, and frequent hand washing.
- Growing evidence shows vitamin D deficiency is common in people with COVID-19.
- Vitamin D appears to be a safe and effective intervention for preventing COVID-19 complications.
- Supplementation may be more effective in those with established deficiencies. Moreover, those who cannot get enough sun exposure should consider taking a supplement.
Reflective of much in life, there is no one answer here.
Based upon the above, I feel strongly and confidently in concluding that there is a positive benefit, both in terms of reducing infection and in terms of reducing severity of infection, to vitamin D supplementation (unless levels are already adequate).
I find the “Swiss cheese approach” to be the most effective as we continue to live, learn, and adapt to life during a pandemic. The Swiss cheese approach posits a layered approach, where with enough layers—all of which have holes—we largely eliminate anything from passing through.
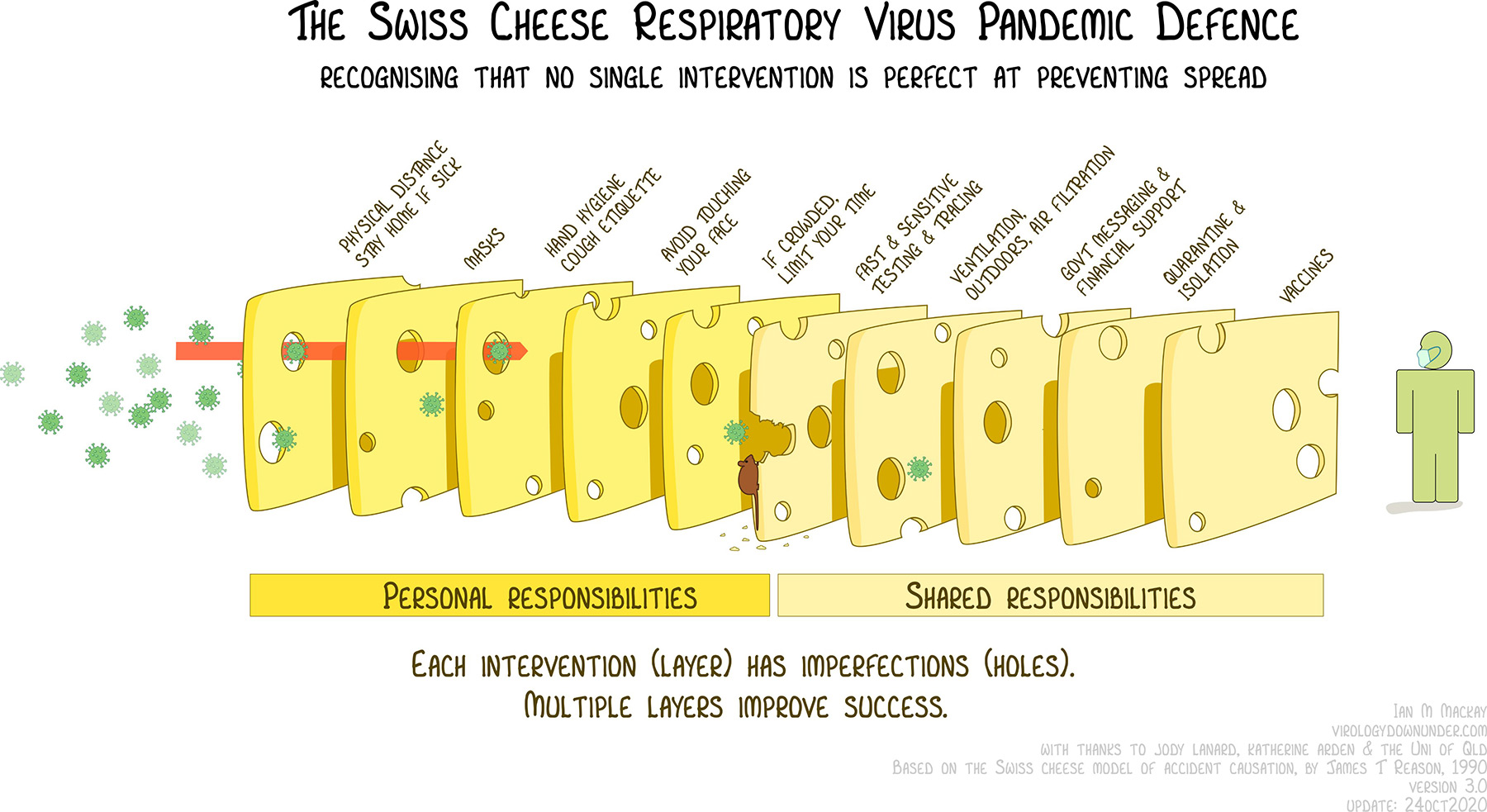
Vitamin D is one of those layers.
COVID-19 and Vitamin D FAQs
Question – Does vitamin D cure or treat COVID-19?
Answer – There is no cure or vaccine for COVID-19. Available evidence shows that the vitamin may help reduce susceptibility to upper respiratory infections.
Question – What is the recommended dose of vitamin D for COVID-19?
Answer – Experts believe a daily dose of 1,000 IU to 4,000 IU should be enough for protection against COVID-19.
Question – How much vitamin D should I take if I am at a higher risk for COVID-19?
Answer – You may consider taking 10,000 IU per day of vitamin D3 for a few weeks, followed by 5000 IU per day.
Question – Can high (mega) doses of vitamin D for COVID-19 cause overdose or toxicity?
Answer – Vitamin D toxicity is extremely rare, and daily doses up to 20,000 IU of vitamin D3 have not been shown to cause toxicity. That said, vitamin D toxicity is potentially serious.
Question – What are the symptoms of vitamin D overdose or of vitamin D toxicity?
Answer – As noted, vitamin D toxicity (overdose) is extremely rare, and the side effects of vitamin D toxicity are uncommon. Toxicity may cause:
- Fatigue;
- Headache;
- Loss of appetite;
- Dry mouth;
- Taste changes;
- Nausea and vomiting.
Further Reading and Selected Resources
- Analysis of vitamin D level among asymptomatic and critically ill COVID-19 patients and its correlation with inflammatory markers. Scientific Reports.
- Association of Vitamin D Status and Other Clinical Characteristics With COVID-19 Test Results. JAMA Network (American Medical Association).
- Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study. The Journal of Steroid Biochemistry and Molecular Biology.
- Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. PLOS ONE.
- Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths. Nutrients.
- MECHANISMS IN ENDOCRINOLOGY: Vitamin D and COVID-19. European Journal of Endocrinology.
- Repairing Low Vitamin D. How to Restore Vitamin D Levels: Expert Guidelines Explained (RAW Forest Foods).
- SARS-CoV-2 positivity rates associated with circulating 25-hydroxyvitamin D levels. PLOS ONE.
- Vitamin C levels in patients with SARS-CoV-2-associated acute respiratory distress syndrome. Critical Care.
- Vitamin D deficiency as risk factor for severe COVID-19: a convergence of two pandemics. MedRxiv (Preprint for Health Sciences).
- Vitamin D sufficiency, a serum 25-hydroxyvitamin D at least 30 ng/mL reduced risk for adverse clinical outcomes in patients with COVID-19 infection. PLOS ONE.
Last updated November 23, 2020.
Recent Posts

Entering the Year of the Horse
Intention With Tenacity From where I sit and write to you here in northern Vermont, the Gregorian Ne...

Chinese Dietary Therapy for the Winter Season
Living—and Eating—Seasonally in the Winter Officially, winter begins here in the Northern Hemisphe...

Chinese Dietary Therapy for the Autumn Season
Living—and Eating—Seasonally in the Autumn Today—September 22, 2025—marks the official start of fa...

An Update On Our Arrow of Eros Vital Fire Elixir Tincture
The Background Behind Its Sudden Disappearance If you’ve been searching for our Arrow of Eros Vital...

Understanding Shilajit: Mineral Medicine of the Mountains
Ancestral Knowledge, Timeless Resilience, and the Quiet Power of Slow Restoration Mountain Manna Ra...

Wèi Qì and Emotional Immunity
Wèi Qì as Emotional Immunity: Resilience, Boundaries, and Inner Strength Wèi Qì is the body’s first...
Site Disclaimers
General Guidence
The content on this site is provided for educational and informational purposes only and should not be construed as medical advice. Always consult a qualified healthcare provider before making changes to your diet, lifestyle, or health regimen, particularly if you are pregnant or nursing, under the age of 18, managing allergies or known sensitivities, or living with any medical conditions.
At RAW Forest Foods, your safety is our priority. Please note that our products are dietary supplements, not medications. The following disclaimer applies:
* These statements have not been evaluated by the Food and Drug Administration. These products are not intended to diagnose, treat, cure, or prevent any disease.
Ingredient Transparency and Allergen Awareness
We are committed to providing transparent ingredient information to help you make informed decisions. If you have or suspect you have allergies to any of our ingredients, we strongly advise against using our products, as allergic reactions can be severe.
Interaction with Medications
If you are taking any medications, consult with your healthcare provider before using supplements. Certain supplements may interact with medications, potentially altering their effectiveness or causing unwanted effects.
For more details, please review our full Terms and Conditions.